A Guide to Filling Out the Yokohama City Cervical Cancer Screening Questionnaire(for 30~60y-old women)
A Guide to Filling Out the Yokohama City Cervical Cancer Screening Questionnaire
For English speakers undergoing a cervical cancer screening in Yokohama City.
This guide explains how to fill out the medical questionnaire for the Yokohama City Cervical Cancer Screening. With English translations and sample images, we hope to make the process smooth even for those unfamiliar with Japanese.
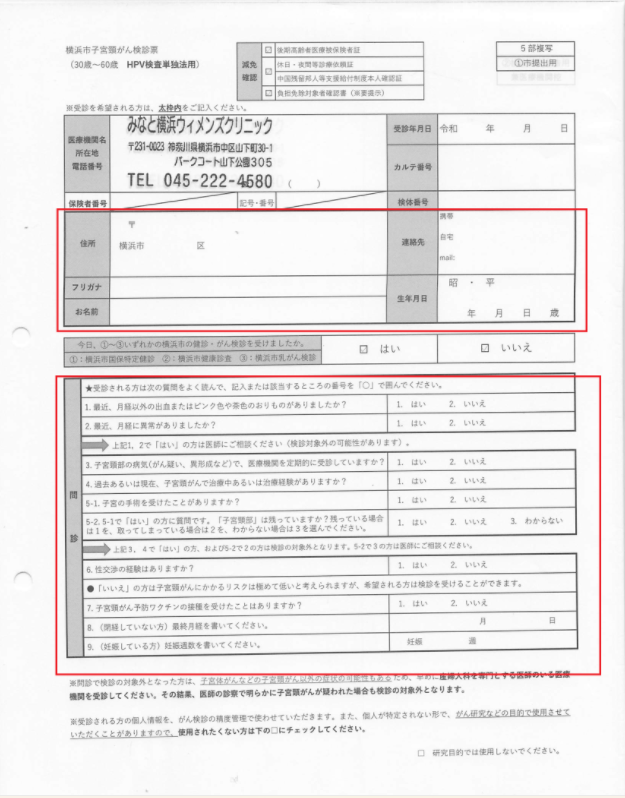
The Complete Questionnaire
This is the questionnaire you will need to fill out. It is mainly divided into two parts: “Personal Information” and “Medical Questionnaire”.
Part 1: Personal Information
First, please fill in your personal information in the top half of the form.
(Sample: Top part of the form)
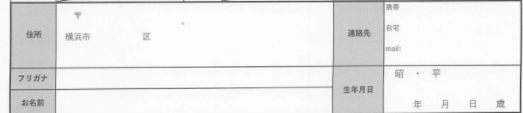
- 1. 住所 (Jūsho): Your Address.
- 2. フリガナ (Furigana): Your Name in Katakana (phonetic script).
- 3. お名前 (Onamae): Your Name.
- 4. 生年月日 (Seinengappi): Your Date of Birth (Year / Month / Day).
- 5. 連絡先 (Renrakusaki): Your Contact Phone Number.
Part 2: Medical Questionnaire (問診)
Next, please answer the questions in the bottom half of the form.
(Sample: Bottom part of the form)
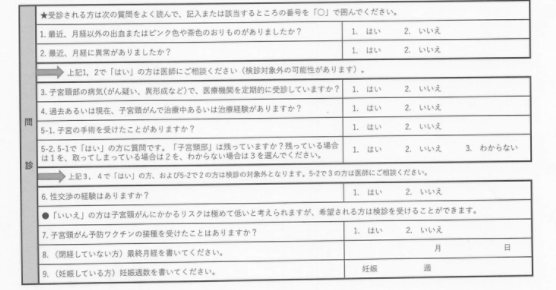
Please read the questions carefully and circle either “1. はい (Yes)” or “2. いいえ (No)”.
1. 最近、月経以外の出血またはピンク色や茶色のおりものがありましたか?
Recently, have you had any bleeding, pinkish, or brownish discharge outside of your menstrual period?
2. 最近、月経に異常がありましたか?
Have you had any abnormalities with your recent menstrual periods?
上記 1、2で「はい」の方は、検診の対象外の可能性がありますので医師にご相談ください。
If you answered “Yes” to questions 1 or 2, please consult with the doctor as you may not be eligible for this screening.
3. 子宮頸部の病気(がん疑い、異形成など)で、医療機関を定期的に受診していますか?
Are you currently receiving regular medical check-ups for any cervical conditions (e.g., suspected cancer, dysplasia)?
4. 過去あるいは現在、子宮頸がんで治療中あるいは治療経験がありますか?
Have you ever been treated for, or are you currently undergoing treatment for, cervical cancer?
5. 子宮の手術を受けたことがありますか?
Have you ever had uterine surgery?
5-1で「はい」の方への質問です。「子宮頸部」は残っていますか?
Do you still have your cervix?
- 1. はい (Yes)
- 2. いいえ (No)
- 3. わからない (I don’t know)
上記 3、4、5-1で「はい」の方、および 5-2で「いいえ」の方は検診の対象外となります。5-2で「わからない」の方は医師にご相談ください。
If you answered “Yes” to questions 3, 4, or 5-1 and “No” to 5-2, you are not eligible for this screening. If you answered “I don’t know” for 5-2, please consult with the doctor.
6. 性交渉の経験はありますか?
7. 子宮頸がん予防ワクチンの接種を受けたことはありますか?
Have you received the HPV vaccine for cervical cancer prevention?
8. (閉経していない方)最終月経を書いてください。
(For those who have not reached menopause) Please write down the date of your last menstrual period. (Month / Day)
9. (妊娠している方)妊娠週数を書いてください。
(For those who are pregnant) Please write down the number of weeks of your pregnancy. (Weeks pregnant)