How to Fill Out Yokohama City Breast/ Cervical Cancer Screening Forms: A Guide for English Speakers
Navigating paperwork at a clinic in Japan can feel a little daunting, especially when everything is in Japanese. But don’t worry! If you’re going for a cervical cancer screening in Yokohama, we’ve got you covered.
This guide will walk you through exactly how to fill out the screening form, step by step.
① Yokohama City Cervical Cancer Screening Form (20-29y-old / 60+y-old Women)
Step 1: The Big Picture
First, let’s look at the entire form. It might seem like a lot, but the good news is you only need to fill out the sections inside the large, bold-lined box. The clinic staff will handle the rest.
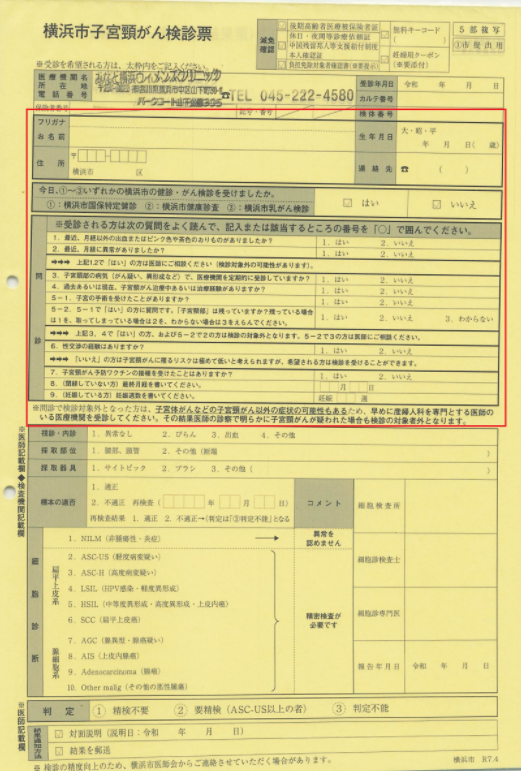
You only need to write in the area inside the bold-lined box.
Step 2: Your Personal Information
Now, let’s zoom in on the top part. This is where you’ll write your personal details.

1. お名前 (O-namae): Name
Write your full name here.
2. 生年月日 (Sei-nen-gappi): Date of Birth
Write your date of birth. The format is often based on the Japanese era, but writing it in the Western format (Year/Month/Day) is usually fine.
3. 住所 (Juusho): Address
Write your current address in Yokohama.
4. 連絡先 (Renraku-saki): Contact Number
Write your phone number where the clinic can reach you.
Right below your contact info, you’ll see this question:
今日、いずれかの横浜市の健診・がん検診を受けましたか。
(Have you undergone any other Yokohama City health check-ups or cancer screenings today?)
Circle はい (Yes) or いいえ (No).
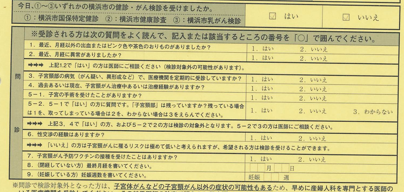
Step 3: The Medical Questionnaire (問診 – Monshin)
Finally, let’s tackle the questionnaire section at the bottom. Just circle the number that corresponds to your answer. `1` is for Yes (はい), and `2` is for No (いいえ).
1. 過去6ヶ月以内に不正出血(月経以外の出血や茶色いおりもの)がありましたか?
Have you had any abnormal bleeding (bleeding other than your period, or brown discharge) in the last 6 months?
2. 最近、月経に異常がありましたか?
Have you had any menstrual irregularities recently?
→→→上記1と2で「はい」の方は医師にご相談ください。
This is a note: If you answered “Yes” to questions 1 or 2, please consult with the doctor.
3. 子宮頸部の病気(がん疑い、異形成など)で、医療機関を定期的に受診していますか?
Are you regularly visiting a medical institution for a cervical condition (suspected cancer, dysplasia, etc.)?
4. 子宮体部の病気で、医療機関を定期的に受診したり治療を受けていますか?
Are you regularly visiting a medical institution or receiving treatment for an endometrial (uterine body) condition?
5-1. 子宮の手術を受けたことがありますか? (Have you ever had uterine surgery?)
5-2「はい」の方へ: 「子宮頸部」は残っていますか? (For those who answered “Yes”at 5-1: Do you still have your cervix?)
1: はい (Yes), 2: いいえ (No), 3: わからない (I don’t know)
→→→上記3,4で「はい」のかた、および5-2で2の方は検査対象外となります。
This is a note:If you answered ‘Yes’ to questions 3 or 4, or answered ‘2’ for question 5-2, you are not eligible for this examination.
6. 性交交渉の経験はありますか?
Have you ever had sexual intercourse?
→→→「いいえ」の方は子宮頸がんを罹るリスクは極めて低いと考えられますが、希望される方は検診を受けることができます。 If you answered “No” to question 7, your risk of developing cervical cancer is considered extremely low, but you can still choose to undergo the screening if you wish.
7.子宮頸がん予防ワクチンの接種を受けたことはありますか?(Have you ever had the HPV vaccine?)
8.(閉経していない方)最終月経を書いてください。月 日(If you are not menopausal, please provide the date of your last menstrual period)Month/date
9. 妊娠している方 (For those who are pregnant)
This question asks if you are pregnant and, if so, how many weeks along you are. If not pregnant, leave it blank.
妊娠 (Pregnancy): __ 週 (weeks)
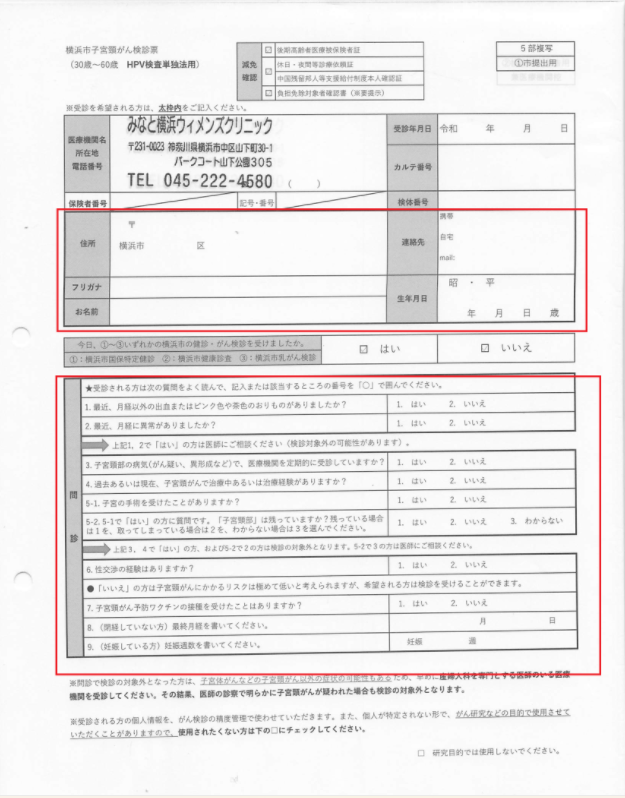
② Yokohama City Cervical Cancer Screening Form (for 30-60y-old women)
The Complete Questionnaire
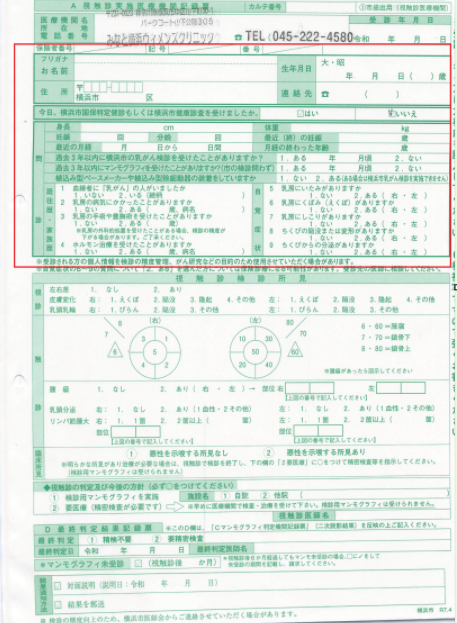
This is the questionnaire you will need to fill out. It is mainly divided into two parts: “Personal Information” and “Medical Questionnaire”.
Part 1: Personal Information
First, please fill in your personal information in the top half of the form.
(Sample: Top part of the form)
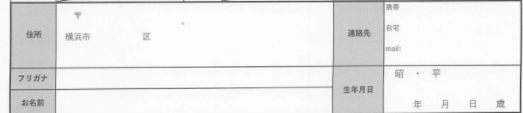
- 1. 住所 (Jūsho): Your Address.
- 2. フリガナ (Furigana): Your Name in Katakana (phonetic script).
- 3. お名前 (Onamae): Your Name.
- 4. 生年月日 (Seinengappi): Your Date of Birth (Year / Month / Day).
- 5. 連絡先 (Renrakusaki): Your Contact Phone Number.
Part 2: Medical Questionnaire (問診)
Next, please answer the questions in the bottom half of the form.
(Sample: Bottom part of the form)
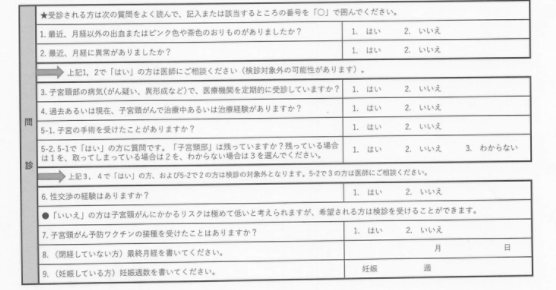
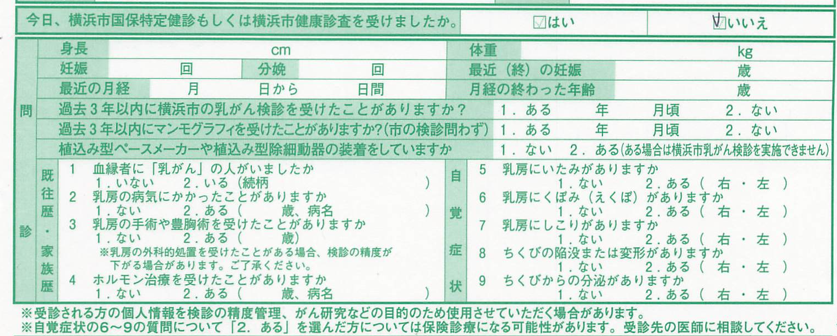
Please read the questions carefully and circle either “1. はい (Yes)” or “2. いいえ (No)”.
1. 最近、月経以外の出血またはピンク色や茶色のおりものがありましたか?
Recently, have you had any bleeding, pinkish, or brownish discharge outside of your menstrual period?
2. 最近、月経に異常がありましたか?
Have you had any abnormalities with your recent menstrual periods?
If you answered “Yes” to questions 1 or 2, please consult with the doctor as you may not be eligible for this screening.
3. 子宮頸部の病気(がん疑い、異形成など)で、医療機関を定期的に受診していますか?
Are you currently receiving regular medical check-ups for any cervical conditions (e.g., suspected cancer, dysplasia)?
4. 過去あるいは現在、子宮頸がんで治療中あるいは治療経験がありますか?
Have you ever been treated for, or are you currently undergoing treatment for, cervical cancer?
5. 子宮の手術を受けたことがありますか?
Have you ever had uterine surgery?
5-1で「はい」の方への質問です。「子宮頸部」は残っていますか? Do you still have your cervix?
- 1. はい (Yes)
- 2. いいえ (No)
- 3. わからない (I don’t know)
If you answered “Yes” to questions 3, 4, or 5-1 and “No” to 5-2, you are not eligible for this screening. If you answered “I don’t know” for 5-2, please consult with the doctor.
6. 性交渉の経験はありますか?
7. 子宮頸がん予防ワクチンの接種を受けたことはありますか?
Have you received the HPV vaccine for cervical cancer prevention?
8. (閉経していない方)最終月経を書いてください。
(For those who have not reached menopause) Please write down the date of your last menstrual period. (Month / Day)
9. (妊娠している方)妊娠週数を書いてください。
(For those who are pregnant) Please write down the number of weeks of your pregnancy. (Weeks pregnant)
③ Yokohama City Breast Cancer Screening Form
Full View of the Form
This is the entire form you will be filling out. The steps below explain how to fill in each section.
Step 1: Personal Information
Please fill in your personal details in the top section of the form.
- お名前(Name)
姓・名の順でご記入ください。(Please write your family name, then given name.)
- フリガナ(Furigana)
カタカナで名前の読み方を書きます。(Write the pronunciation of your name in Katakana.)
- 生年月日(Date of Birth)
和暦(大正・昭和・平成)に◯をつけ、年月日を記入します。(Circle the era name and write your birth year, month, and day.)
- 年齢(Age)
- 住所(Address)
- 連絡先(Contact Number)
電話番号をご記入ください。(Your phone number.)
【記入箇所 / Area to fill】

Step 2: 問診Medical Questionnaire
【Area to fill】
。 Please answer the questions in the large central box. Circle the number that applies to you.
既往歴・家族歴
Medical & Family History
- 妊娠・分娩・身長・体重(Pregnancy, Deliveries, Height, Weight)
- 最近の月経・閉経(Most recent period / Menopause)
- 過去3年以内に横浜市乳がん検診を受けたか(Had Yokohama breast screening in last 3 years?)
- 3年以内にマンモグラフィを受けたか(Had a mammogram in the last 3 year?)
- ペースメーカー等の装着(Have a pacemaker, etc.?)
- 1.血縁者に「乳がん」の人がいるか(4. Blood relatives with breast cancer?)
- 2. 乳房の病気にかかったことがあるか(2. Ever had other breast diseases?)
- 3. 乳房の手術や豊胸術を受けたか(3. Ever had breast surgery or augmentation?)
- 4. ホルモン治療を受けたことがあるか(4. Ever had hormone therapy?)
自覚症状
Current Symptoms
- 5. 乳房にいたみがあるか(5. Have pain in your breast?)
- 6. 乳房にくぼみ(ひきつれ)があるか(6. Have dimpling in your breast?)
- 7. 乳房にしこりがあるか(7. Have a lump on your breast?)
- 8. ちくびの陥没や変形があるか(8. Have an inverted nipple?)
- 9. ちくびからの分泌物があるか(9. Have nipple discharge?)
(About the Choices)
For most questions, you will have the following choices:
- 1. ない(1. No / I don’t have it)
- 2. ある(2. Yes / I have it) – もし「ある」場合、(右・左 / Right・Left) のどちらかもお答えください。(If yes, please also indicate Right or Left.)